To view the original Medscape article, click here
Hello. I am Dr. Tom Chiller, a medical epidemiologist at the Centers for Disease Control and Prevention (CDC). Today I am pleased to speak as part of the CDC Expert Video Commentary Series on Medscape.
As you probably are well aware, CDC, in collaboration with state and local health departments and the US Food and Drug Administration (FDA), is investigating a multistate fungal meningitis outbreak among patients who received contaminated steroid injections.
Several patients have suffered from strokes that are believed to have resulted from their infections. This investigation also includes possible fungal infections associated with injections into peripheral joints, such as a knees, shoulders, or ankles.
To date, all identified cases associated with this outbreak have received at least 1 of 3 lots of preservative-free methylprednisolone acetate (MPA) from the New England Compounding Center (NECC).
The fungal infections we are seeing associated with this outbreak are extremely rare. CDC has convened a panel of the nation’s leading clinical fungal experts who are working with us to ensure that our diagnostic and treatment guidance is appropriate for identifying and treating patients who develop infections.
Today I want to give you an update on where we stand with respect to our clinical guidance.
First, here is what we know: To date, more than 300 cases have been reported to us, which includes 24 deaths across 17 states.
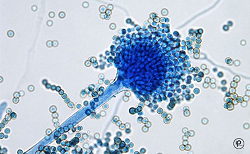
Of cases in which we have identified a fungus, most have been Exserohilum rostratum. One patient has been found to be infected with Aspergillus fumigatus and another with a Cladosporium species. These fungi are common in the environment but were not a recognized cause of meningitis before this outbreak. We are really in new territory when it comes to treatment and management of patients with Exserohilum infection.
CDC and FDA have also confirmed the presence of Exserohilum in 2 of the 3 unopened vials of MPA. We continue to test the third implicated lot of MPA as well as other NECC medications.
Of the approximately 14,000 patients who received injections from 1 of the 3 contaminated lots of MPA, nearly all have been contacted for further follow-up. Among people with meningitis for whom we have clinical information available, the onset of symptoms is typically 1-4 weeks following injection. However, we know that fungal infections can be slow to develop and that there are reports of longer periods of time between injection and onset of symptoms, so we need to monitor these patients for development of signs and symptoms for several months following the injection.
For patients who received epidural or paraspinal steroid injections with medication from any of the 3 recalled lots of MPA, we need to carefully clinically evaluate them. If they have any symptoms consistent with meningitis or posterior circulation stroke, cerebrospinal fluid (CSF) should be obtained for diagnosis unless contraindicated. We also encourage physicians to have a low threshold to obtain CSF in patients with mild signs and symptoms of meningitis because we are aware that some patients in this outbreak have presented with minimal symptoms. When obtaining CSF for diagnosis, we encourage that this be done at a site other than the site used for the steroid injection when possible.
At this time, CDC does not recommend initiation of antifungal treatment in people who received a contaminated steroid injection but who do not have any symptoms or in whom there is no laboratory evidence of infection. However, some patients may be at greater risk than others of developing fungal meningitis. Specific CDC analysis has shown that the greatest risk is in the first 6 weeks after injections.
Clinicians may consider the option of obtaining CSF in patients who received their last injection within the past 6 weeks (42 days) to look for evidence of meningitis before symptoms appear. From our analysis, we have seen that the more time that has passed since the date of the steroid injection, the lower the risk of developing disease.
For patients who are presenting with joint infections, clinicians should collect synovial fluid and/or synovial tissue, either by arthrocentesis or biopsy, and look for evidence of infection.
Let’s shift gears and talk about treatment. If you have a patient who has evidence of fungal meningitis or joint infection, make sure you are following CDC’s treatment recommendations.
At this time, CDC is recommending voriconazole, which is an effective agent for treating infections due to brown-black molds, such as Exserohilum, as well as infections due to Aspergillus species, and has good penetration into the central nervous system.
CDC continues to consult with national experts about treatment options for infections associated with this outbreak. As more information becomes available on patient management, we will continue to update the clinical community.
Please see the links below to stay up to date on the latest CDC guidance.
Finally, because this is an ongoing investigation, we continue to need your help. If you see patients with any suspected adverse events following use of NECC products, please report this to your state health department and FDA’s MedWatch program at 1-800-332-1088 or FDA.gov/medwatch.
Thank you.
Medical and Patient education videos
-
Title
Description
-

I have Sarcoidosis, Chronic Pulmonary Aspergillosis (CPA) and a very low CD4 count. I have challenged myself to do a daily vlog for 30 days
Follow me on twitter @StewArmstrong
Here is the link for all of the monthly aspergillosis meetings http://www.nacpatients.org.uk/monthly…
This meeting was for July 2016.
Aspergillus Website: Follow all of our Youtube collections here
-

Stewart Armstrong has chronic pulmonary aspergillosis and has undertaken to record a video of every day of his life for a month in order to help raise awareness of aspergillosis and how it impacts their daily lives.
These videos are interesting for a number of reasons – not least because patients often say that they don’t look unwell so many people don’t understand how serious aspergillosis is. Does Stewart look or act unwell?
See the month of vlogs in the playlist below, or go to Stewart’s YouTube page to watch more of his videos.
-
Global fungal killers and life-threatening infections
Fungi are everywhere, and a few species can cause very serious lethal infections. Fungal infections
-

This panel considers and debates one of the greatest obstacles to food security in many parts of the world: mycotoxin. Aflatoxin is a particularly dangerous mycotoxin produced predominantly by two Aspergillus fungi. It colonizes a variety of important food and feed crops both pre- and post-harvest, including groundnuts, tree nuts, maize, rice, figs and other dried foods, spices, crude vegetable oils and cocoa. Contaminated crops have significant health risks for both humans and animals, having been linked to retarded growth and development (stunting), immunosuppression and liver cancer. The aflatoxin issue has other, complex implications for food security and, by limiting farmers’ access to international markets, can lead to food waste and economic instability.
Panelists:
-John Lamb, Principal Associate, Abt Associates
-Dr. Kitty Cardwell, National Program Leader, USDA-NIFA
-Barbara Stinson, Senior Partner, Meridian Institute; Project Director, Partnership for Aflatoxin Control in Africa
-Moderator: Dr. Howard-Yana Shapiro, Chief Agricultural Officer, Mars, Incorporated -

The role of poorly maintained ventilation ductwork in spreading airborne infections is largely ignored because it is ‘out of sight out of mind’, but recent analysis by healthcare professionals confirms that the risks are increasing.
Ghasson Shabha will identify particular threats in healthcare facilities from dirty ductwork. He also points out that fewer than 5% of building air-conditioning systems have been inspected despite regulations making this mandatory. Dr Shabha will look at how planned cleaning strategies can reduce risks and how hospitals can use 3D building information modelling software to identify ‘infection hotspots’.
The healthcare environment can be described as a reservoir for potentially infective agents which can spread unpredictably in a whole array of ways particularly in ventilation and air-conditioning systems making it difficult to effectively control and manage, for those seeking timely information about the patterns of cross-infection. The severity of the problem has been highlighted extensively over the past decade, as part of wider umbrella of what was known as health care acquired infections (HCAIs). Airborne transmission extends over a wide spectrum, and includes many prevalent agents, inter alia Mycobacterium tuberculosis (TB),nosocomial MRSA, Aspergillus fumigatus, Serratia marcescens, norovirus, and other airborne infection.
Dr Shabha was speaking live from Birmingham and this CIBSE ASHRAE Group (cibseashrae.org) webinar was co-sponsored by the B&ES Ventilation Hygiene Group and the Institute of Healthcare Engineering and Estate Management (IHEEM).
-

Oliphant Science Awards – Year 1 project by Haruki Kurioka, Aleksa Novakovic and Bogdan Novakovic (St Andrew’s Primary School, Adelaide)
Food that we consume daily is rich in good bacteria and fungi. Yogurt, Yakult and Natto (fermented soybeans) are rich in bacteria. Cheeses (e.g. Brie & Blue cheese) and Koji contain fungi Penicillium and Aspergillus, respectively. Many Japanese and continental seasonings and dishes can be prepared with those products. Many kids and their parents don’t know much about good bacteria and fungi. First year students are here to tell us their story. Enjoy it!



){kind=link}