To view the original Medscape article, click here
Hello. I am Dr. Tom Chiller, a medical epidemiologist at the Centers for Disease Control and Prevention (CDC). Today I am pleased to speak as part of the CDC Expert Video Commentary Series on Medscape.
As you probably are well aware, CDC, in collaboration with state and local health departments and the US Food and Drug Administration (FDA), is investigating a multistate fungal meningitis outbreak among patients who received contaminated steroid injections.
Several patients have suffered from strokes that are believed to have resulted from their infections. This investigation also includes possible fungal infections associated with injections into peripheral joints, such as a knees, shoulders, or ankles.
To date, all identified cases associated with this outbreak have received at least 1 of 3 lots of preservative-free methylprednisolone acetate (MPA) from the New England Compounding Center (NECC).
The fungal infections we are seeing associated with this outbreak are extremely rare. CDC has convened a panel of the nation’s leading clinical fungal experts who are working with us to ensure that our diagnostic and treatment guidance is appropriate for identifying and treating patients who develop infections.
Today I want to give you an update on where we stand with respect to our clinical guidance.
First, here is what we know: To date, more than 300 cases have been reported to us, which includes 24 deaths across 17 states.
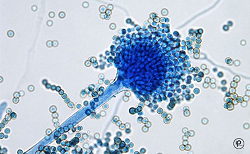
Of cases in which we have identified a fungus, most have been Exserohilum rostratum. One patient has been found to be infected with Aspergillus fumigatus and another with a Cladosporium species. These fungi are common in the environment but were not a recognized cause of meningitis before this outbreak. We are really in new territory when it comes to treatment and management of patients with Exserohilum infection.
CDC and FDA have also confirmed the presence of Exserohilum in 2 of the 3 unopened vials of MPA. We continue to test the third implicated lot of MPA as well as other NECC medications.
Of the approximately 14,000 patients who received injections from 1 of the 3 contaminated lots of MPA, nearly all have been contacted for further follow-up. Among people with meningitis for whom we have clinical information available, the onset of symptoms is typically 1-4 weeks following injection. However, we know that fungal infections can be slow to develop and that there are reports of longer periods of time between injection and onset of symptoms, so we need to monitor these patients for development of signs and symptoms for several months following the injection.
For patients who received epidural or paraspinal steroid injections with medication from any of the 3 recalled lots of MPA, we need to carefully clinically evaluate them. If they have any symptoms consistent with meningitis or posterior circulation stroke, cerebrospinal fluid (CSF) should be obtained for diagnosis unless contraindicated. We also encourage physicians to have a low threshold to obtain CSF in patients with mild signs and symptoms of meningitis because we are aware that some patients in this outbreak have presented with minimal symptoms. When obtaining CSF for diagnosis, we encourage that this be done at a site other than the site used for the steroid injection when possible.
At this time, CDC does not recommend initiation of antifungal treatment in people who received a contaminated steroid injection but who do not have any symptoms or in whom there is no laboratory evidence of infection. However, some patients may be at greater risk than others of developing fungal meningitis. Specific CDC analysis has shown that the greatest risk is in the first 6 weeks after injections.
Clinicians may consider the option of obtaining CSF in patients who received their last injection within the past 6 weeks (42 days) to look for evidence of meningitis before symptoms appear. From our analysis, we have seen that the more time that has passed since the date of the steroid injection, the lower the risk of developing disease.
For patients who are presenting with joint infections, clinicians should collect synovial fluid and/or synovial tissue, either by arthrocentesis or biopsy, and look for evidence of infection.
Let’s shift gears and talk about treatment. If you have a patient who has evidence of fungal meningitis or joint infection, make sure you are following CDC’s treatment recommendations.
At this time, CDC is recommending voriconazole, which is an effective agent for treating infections due to brown-black molds, such as Exserohilum, as well as infections due to Aspergillus species, and has good penetration into the central nervous system.
CDC continues to consult with national experts about treatment options for infections associated with this outbreak. As more information becomes available on patient management, we will continue to update the clinical community.
Please see the links below to stay up to date on the latest CDC guidance.
Finally, because this is an ongoing investigation, we continue to need your help. If you see patients with any suspected adverse events following use of NECC products, please report this to your state health department and FDA’s MedWatch program at 1-800-332-1088 or FDA.gov/medwatch.
Thank you.
Medical and Patient education videos
-
Title
Description
-
Prof. Patricia Muñoz, Division of Clinical Microbiology and Infectious Disease, Hospital General Universitario Gregorio Marañón, Madrid, Spain
-
Dr. Eavan Muldoon, Consultant in Infectious Diseases, University Hospital of South Manchester
-
Prof. Adilia Warris, Principal Investigator, Aberdeen Fungal Group, University of Aberdeen
-
Created by Patrick Hickey for the “Killer Fungus” exhibit at the 2016 Royal Society Summer Science Exhibition
A large dish of nutrient jelly inoculated with several different fungal species and then filmed over 5 days. The different colours of the fungal species used gradually grow to form the image and spell out the message ‘Killer fungus’.
The awareness, diagnosis and treatment of serious fungal infections needs dramatic improvement throughout the world as millions die needlessly every year.
The Royal Society Summer Exhitions are aimed at informing and inspiring the public – children and our future engineers and scientists in particular. Killer fungus is one exhibit amongst many more covering every aspect of science you can think of!
More
http://www.killerfungus.org/ h
ttps://twitter.com/ killerfungus16 https://www.facebook.com/ killerfungus16/ -
Fungi are everywhere. They’re present in the air, in our food, some even live inside our bodies. But most of us rarely think about diseases caused by fungi. This is because our defences do a really good job in keeping them in check.
However for millions of people whose immune system are defective fungi can cause serious infections that are hard to treat and can be life threatening.
A group of cells called phagocytes play a key role in keeping us safe from fungi. They normally patrol our body so when there’s a breach they are the first to respond. Their function is to seek eat and destroy microbial intruders.
But no all fungi are alike. My Ph.D. project aims to understand how phagocytes tackle such different targets. So far I have found there are huge differences in the rate at which various different fungi are engulfed by phagocytes.
The speed of these processes depends on the chemical composition of the fungi, whether they are alive or dead, and whether they are coated with human proteins that help to mark them as intruders.
Understanding the basic biology behind these processes is the first step towards developing new treatment strategies.
Maria Fernanda Alonso works in Professor Neil Gow’s lab at the University of Aberdeen.
-

Candida albicans is one of the fungal species most commonly causing life threatening infections in vulnerable patients. Our group is studying the mitochondria in Candida albicans cells.
Just like in our cells the mitochondria are the batteries of the cell, producing energy required for growth and in fungal cells can also influence infection.
The mitochondria can influence components of the fungal cell wall and its ability to infect us.
If we understand how mitochondria are influencing these factors, we can develop new anti-fungals or we can use existing anti-fungals in new combinations in order to tackle life threatening infections.
Lucian Duvenage works in Dr Campbell Gourlay’s lab at the University of Kent
-

Every day we inhale hundreds of fungal spores but these in healthy individuals are efficiently eliminated by specialist immune cells called phagocytes which engulf and kill them. However, some human illnesses interfere with this defence mechanism, increasing susceptibility to fungal diseases.
A specialist lung tissue called the epithelium is the first line of contact between the inhaled spores and us, the host. We are working to understand how the lung epithelium interacts with the spores of a common mould called Aspergillus fumigatus.
We have generated fluorescent Aspergillus and combined this with fungal and host specific dyes to directly visulaise this interaction. We have discovered that epithelial cells ingest fungal spores and kill them.
This might provide a critical defence mechanism which is acting while we breathe, and before even phagocytes arrive at the site of the infection.
We are now trying to work out how epithelial cells grab and ingest fungal spores, by using fluorescent fungal mutants and targeted elimination of host proteins.
Once we understand this process in detail we can design new therapies to assist a quicker elimination of the dangerous fungal spores we all inhale on a daily basis.
Dr Margherita Bertuzzi works in Dr Elaine Bignell’s lab at the University of Manchester
-

My research is focused on infections caused by Aspergillus, which is present in the environment all around us. We each inhale hundreds of fungal spores every single day, and for the majority of people this doesn’t cause any problems, but for people whose immune system isn’t working properly Aspergillus can cause serious, even life threatening, infections.
One group of patients who are at particular risk of Aspergillus infection are people with a rare inherited immune deficiency called chronic granulomatous disease, or CGD.
For these patients infection with Aspergillus is frequently fatal, even with appropriate anti-fungal treatment.
My research so far suggests that rather than not mounting a sufficient immune response, the CGD immune system actually over-reacts to Aspergillus, causing significant tissue damage but without clearing the fungal infection.
We’re therefore looking at whether we can use new treatments aimed at reducing inflammation alongside conventional anti-fungal drugs to improve the outcome of these devastating infections for CGD patients.
Dr Jill King works in Professor Adilia Warris’s lab at the University of Aberdeen
-

Cryptococcus, like many fungi, produces spores that are found in the air that we breathe. These spores will be inhaled into our lungs but they do not cause any harm because of our immune defences. However, they can cause life-threatening infections in individuals that have a weakened immune system, for example those that have AIDS or have had an organ transplant.
So, we’re interested in immune cells called macrophages which are needed for immune defence against Cryptococcus.
It is impossible to see how immune cells destroy this fungus during infection because we do not have see-through bodies. So, in order to study this we are using zebrafish. Zebrafish have a similar immune system like our own but are transparent which makes it possible to see how infections happen. Using zebrafish we are testing new ways to enhance immune defences against Cryptococcus.
Ultimately these investigations may lead to development of novel therapies towards Cryptococcal infections.
Alfred Kamuyango works in Professor Simon Johnston’s lab at the University of Sheffield.
-
We can view an infection as a battle between the human host and the microbial invader. The outcome of which decides whether the host remains healthy or succumbs to disease. As this battle rages microbial invaders use their hosts as a source of nutrients.
However, the human body has evolved complex systems to limit access to certain essential nutrients in an attempt to starve the invading microbes and prevent disease.
We call these processes nutritional immunity. Therefore, to win the battle and cause disease microbial pathogens must have evolved strategies to thrive in a nutritionally restrictive environment within its infected host.
We are interested in exploring how the human fungal pathogen Candida albicans adapts to limitations to essential trace nutrient zinc. We have identified specific coping mechanisms that are adopted by this fungus in order to deal with nutritional immunity. In response to zinc starvation,Candida albicans dramatically changed their cell shape.
We therefore want to know how this change is regulated and what impact it has on the progression of infection with the ultimate aim to therapeutically manipulate the system and push the balance back in favour of the human host to prevent disease.
Dhara Malavia works in Dr Duncan Wilson’s lab at the University of Aberdeen.
){kind=link}