Description:
Fungi are everywhere. They’re present in the air, in our food, some even live inside our bodies. But most of us rarely think about diseases caused by fungi. This is because our defences do a really good job in keeping them in check.
However for millions of people whose immune system are defective fungi can cause serious infections that are hard to treat and can be life threatening.
A group of cells called phagocytes play a key role in keeping us safe from fungi. They normally patrol our body so when there’s a breach they are the first to respond. Their function is to seek eat and destroy microbial intruders.
But no all fungi are alike. My Ph.D. project aims to understand how phagocytes tackle such different targets. So far I have found there are huge differences in the rate at which various different fungi are engulfed by phagocytes.
The speed of these processes depends on the chemical composition of the fungi, whether they are alive or dead, and whether they are coated with human proteins that help to mark them as intruders.
Understanding the basic biology behind these processes is the first step towards developing new treatment strategies.
Maria Fernanda Alonso works in Professor Neil Gow’s lab at the University of Aberdeen.
Medical and Patient education videos
-
Title
Description
-

Woodrow Maitland tells of his personal experience of having aspergillosis. Like most people he had never heard of aspergillosis when he was finally diagnosed and treated at the National Aspergillosis Centre, Manchester, UK
-
A series of nasal endoscopies – before during and after surgery. Surgical endoscopy by Raphaella Migliavacca. A patient 12 years old with AML undergoes remission following chemotherapy (2 rounds), admitted several months later with high fever and neutropenia. Patient undergoes regime of antifungal therapy including fluconazole, AmpB and voriconazole. (see full case as powerpoint slides presented In Brazil In FocusVII Aug 2009 Raphaella Migliavacca.). Nasal endoscopy was performed both pre-operatively and surgery removed a fungal ball. Biopsy revealed suppurative acute inflammatory findings (middle turbinate) and angioinvasive fungal structures consistent with aspergillosis. Cultures revealed Aspergillus flavus. Eight weeks later another endoscopy post surgery revealed marked improvement and reduced inflammation. The patient was given 12 weeks voriconazole followinf the surgery, followed by 3rd chemotherapy. The patient had recovered and was in complete remission 4 months after the surgical endoscopy.
-
Pre-operative endoscopy by Raphaella Migliavacca.
-

Produced by David Denning and described by Dr Rob Bissett. With kind permission of Gardiner-Caldwell, funded by Janssen-Cilag. Copyright Aspergillus Website.
-
This patient had a small hole in the bone at the base of the skull. He underwent endoscopy through the nose which shows the defect in the skull through which the brain is visible (pulsating). Kindly provided by Hesham Saleh, Consultant Rhinologist, Charing Cross and Royal Brompton Hospital .
-

The Aspergillus Website maintains a collection of clinical videos published on Youtube. Click on the listing at the top to access all videos.
-

Kindly provided by Hesham Saleh, Consultant Rhinologist, Charing Cross and Royal Brompton Hospital
-

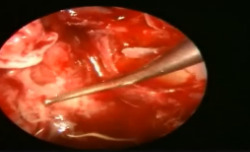
Removing fungal growth from the maxillary sinus via the use of an endoscope.
-

This video shows the removal of the fungal ball through the left nasal passage
-

Produced by Dr Mark Jones and David Denning. Copyright Aspergillus Website.
{kind=link}