Submitted by GAtherton on 16 December 2015
Allergic Bronchopulmonary Aspergillosis (ABPA) is treated using steroid therapy as standard, and more recently alongside antifungal medication (in some cases). Steroids are effective in arresting debilitating degeneration of lung tissue, especially if diagnosed early, and are known to be effective when treating the acute phases of the condition.
However the use of steroid is based on experience rather than clinical trials so the optimal dose for management of ABPA is unknown. The use of high doses of steroid is common but the number of severe side effects caused by long term use of high dose steroids are well described – it would clearly be better if we could limit steroid dose given to these patients.
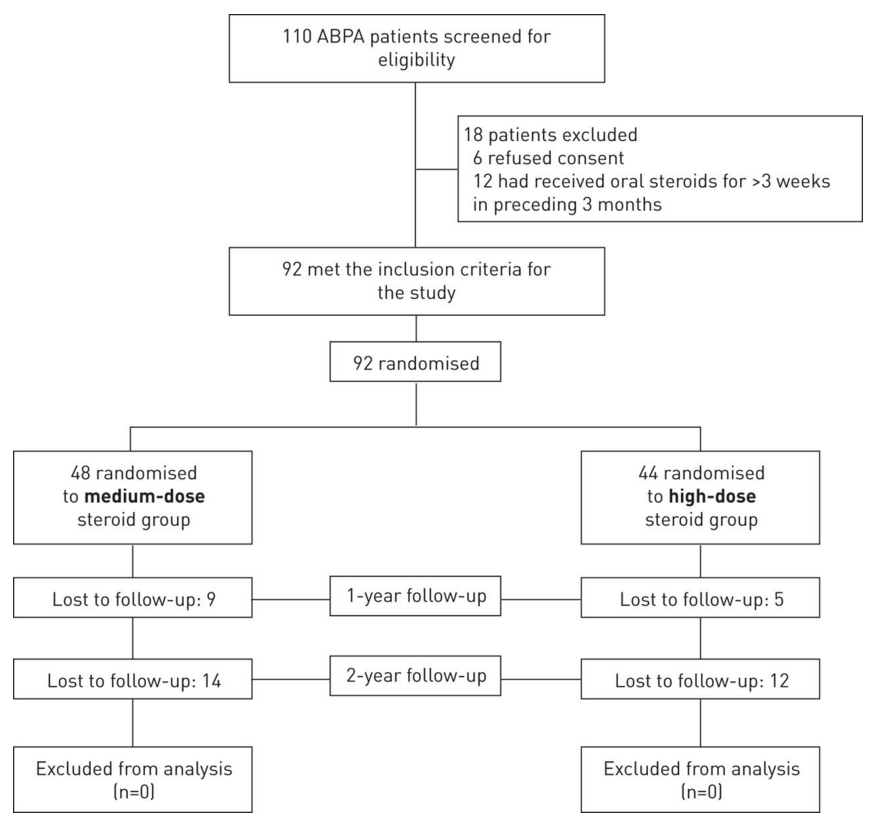
Agawal et. al. (2015) compared outcomes (efficacy and safety) when treating ABPA patients with high dose steroids (0.75 mg·kg−1·day−1 for 6 weeks, then 0.5 mg·kg−1·day−1 for 6 weeks, followed by tapering of 5 mg every 6 weeks to complete a total duration of 6–12 months) versus medium dose steroids (0.5 mg·kg−1·day−1 for 1–2 weeks, then on alternate days for 6–8 weeks, followed by tapering of 5–10 mg every 2 weeks, until discontinuation). They hypothesized initially that high dose steroids will be better than medium dose to prevent exacerbation and progression of ABPA and tested 92 subjects, 44 high dose, 48 medium dose..
However the findings of this trial suggested that medium dose steroid therapy is as good as high dose therapy in preventing exacerbation and steroid-dependence and medium dose is safer in that patients are less prone to toxic side effects. The authors conclude that the high dose steroid strategy should not be the default option for the treatment of early stage acute ABPA, though care must be taken when using the medium dose approach as a few individuals respond less well than most.
News archives
-
Title
Date






 ,
, 



{kind=link}